
The coronavirus disease has spread across the world emerging as a pandemic, traumatising the globe. According to the World Health Organization and the Center for Disease Control and Prevention, older individuals and those with pre-existing medical conditions such as asthma, heart disease or diabetes, seem to be at a higher risk of becoming severely ill from COVID-19.
From several overseas studies, it may be estimated that those who contract COVID-19 and who are 65 years and older have a 4% mortality rate, 75 years and older have an 8% mortality rate, and 85 years and older have a 15% mortality rate, with the average mortality rate being around 2%.
In his speech on 14 April 2020 announcing a 19-day extension of the nationwide lockdown, PM Narendra Modi urged people to give “extra care” to the elderly, especially those with chronic diseases, in tandem with “social distancing” and self-isolation.
The elderly population in India (defined as 60 years or above) is estimated to be around 10.4 crore according to the 2011 Census. Similarly, according to the National Sample Survey 76th Round report on ‘Persons with Disabilities in India’, the disabled population in India is estimated to be 2.6 crore. It takes into consideration the 21 types of disabilities included in the Rights of Persons with Disabilities Act, 2016.
The elderly and Persons with Disabilities (PwD) are some of the most vulnerable sections of society and constitute about one-tenth of the total population of the country. Including the disabled, out of the total older population, 2.1 crores belong to the poorest households having a monthly household income of less than Rs2,900.
These segments are some of the worst-hit in terms of accessibility, availability and affordability of basic lifesaving services, and in being affected by depression and anxiety.
It is now evident that this virus infects people especially with a weak immune system, like the elderly. This calls for an increased and immediate focus on accessible and emergency healthcare, with an emphasis on feasibly practising hygiene and distancing.
This is vital for the susceptible segments of our population that require more and specialised medical attention.
The WHO has published ‘Disability considerations during the COVID-19 outbreak’, highlighting the greater significance of the impact of COVID-19 on the disabled population, which can be mitigated through appropriate action and protective measures by key stakeholders.
Similarly, a statement from the WHO underlines the increased risk to the elderly from COVID-19, and pushes for a collective approach to supporting and protecting older people living alone, with a special attention to be given to those who provide care for them.
The sudden announcement of the lockdown – now extended – in the country led to panic and socioeconomic and health emergencies, wherein the PwD and elderly are among the worst affected. According to the United Nations, unless governments and communities take action, this section will continue to face problems during the COVID-19 pandemic.
The Disabled and Elderly in India: State of Affairs
The ‘Elderly in India’ Report (2016) by the Union Ministry of Statistics and Programme Implementation presents some characteristics of the older population based on data from the 2011 Census and the 2013 Sample Registration System report.
Both the share and size of the elderly population was found to be increasing over time. From 5.6% in 1961 the proportion increased to 8.6% in 2011. For males, it was marginally lower at 8.2%, while for females it was 9.0%. 71% of the elderly population was reported to reside in rural areas and 29 % in urban areas.
The most common disability among the aged persons was locomotor disability and visual disability, with around 5% of the 60+ population having a physical disability.
There are 21 types of disabilities identified under the Rights of Persons with Disabilities Act, 2016 (PwD Act, 2016). These fall under the categories of locomotor disability, visual disability, hearing disability, speech and language disability, mental retardation/ intellectual disability, mental illness, and other disabilities.
The NSS 76th Round report based on this classification finds a prevalence of disability (percentage of PwD in the population) of 2.2% in India, with a higher prevalence in rural areas (2.3%) than in urban areas (2.0%), and higher among males (2.4%) than among females (1.9%). According to the Report, only 28% of the total disabled people have Disability Certificates (which is about only 73 lakh out of 2.6 crore disabled people). Only 21.8% of the individuals receive government aid, 1.8% receive aid from organizations other than government and 76.4% do not receive any aid.
The policy decision of a lockdown is not sensitive to the population of the elderly and PwD in its entirety. According to the two reports, around 4% PwD live alone and 14% of the elderly population is dependent on others (caregivers). Frequent visits to hospitals and rehabilitation centres are often a requirement.
The caregivers – although immensely vital – may be hesitant to provide their services in the current scenario due to the increased risk of infection. When practising a seemingly basic habit of handwashing might be contingent upon the ability to access and use a facility to do so, following other safety guidelines would be similarly conditional, for the segments of the elderly and disabled that are further at risk in isolation.
According to the Ministry of Health and Family Welfare (MoHFW), about 63% of the Coronavirus related deaths are in the age cohort of 60+.
A lack of accessible information and its dissemination, a faulty built-in environment and negative social attitudes towards PwD are matters of grave concern, particularly as these times put their lives and livelihood at serious risk.
Persons with visual disabilities rely highly on the sense of touch (reading Braille, providing inputs on electronic devices, using canes etc) for mobility and work, thus increasing their risk of getting infected.
Many of the quarantine centres don’t have PwD/ elderly friendly infrastructure like lifts or disabled-friendly toilets. This needs to be taken cognizance of and addressed swiftly.
Government Policies, Acts, and the Welfare Framework
The Nodal Union Ministry responsible for senior citizens and PwD is the Ministry for Social Justice and Empowerment (MoSJE). For providing more effective provisions for the elderly, the Maintenance and Welfare of Parents and Senior Citizens Act, 2007 was initiated.
Further, the National Policy for Senior Citizens, 2011 was aimed at the welfare of older persons, and underlined the value of an “age-integrated society”. It laid out eight areas of intervention: income security in old age, healthcare, safety and security, housing, productive ageing, welfare, multi-generational bonding, and media.
The Integrated Programme for Senior Citizens is a significant Central Sector Scheme here. Its main objective is to “improve the quality of life of Senior Citizens by providing basic amenities like shelter, food, medical care and entertainment opportunities and by encouraging productive and active ageing through providing support for capacity building of State/ UT Governments/ Non-Governmental Organizations (NGOs)/ Panchayati Raj Institutions/ local bodies and the community at large.”
The Department for Empowerment of Persons with Disabilities (Divyangjan) under the MoSJE caters to the needs of the disabled communities. It administers three Acts: The Rights of Persons with Disabilities Act, 2016; The National Trust for the Welfare of Persons with Autism, Cerebral Palsy, Mental Retardation and Multiple Disabilities Act, 1999, and the Rehabilitation Council of India Act, 1992.
The National Policy for Persons with Disabilities was released by MoSJE in 2006. It focused on prevention of disabilities, rehabilitation measures (physical strategies, education, economic rehabilitation), women and children with disabilities, a barrier-free environment, social security and other crucial aspects.
The major schemes of the Department include: Assistance to Disabled Persons for Purchase/Fitting of Aids/Appliances (ADIP); Scheme for Implementation of Persons with Disabilities Act (SIPDA); Deendayal Disabled Rehabilitation Scheme (DDRS); Disability Rehabilitation Centres (DDRC); and various fellowships, scholarships and skill trainings for PwD.
In 2018-19, 1.8 lakh beneficiaries availed the benefits of ADIP when the actual budget estimate stood at Rs. 216 crore. In FY2020-21 it has been allocated a fund of Rs. 230 crore. However, it will pass the litmus test only if the resources are channelled into implementation, beyond announcements.
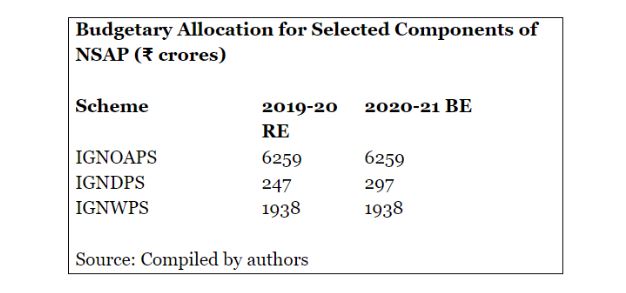
National Social Assistance Program (NSAP) and Other Government Initiatives
The National Social Assistance Program (NSAP) came into effect from 15th August 1995. It introduced assistance for the poor and aims at ensuring a minimum national standard for social assistance in addition to the benefits that states are currently providing or might provide in the future.
It has five sub-schemes as its components: Indira Gandhi National Old Age Pension Scheme (IGNOAPS), Indira Gandhi National Widow Pension Scheme (IGNWPS), Indira Gandhi National Disability Pension Scheme (IGNDPS), National Family Benefit Scheme (NFBS) and Annapurna.
Under this program, around 4 crore beneficiaries have been digitized, in all – including 3.3 crore under central schemes and around 70 lakh beneficiaries under state schemes.
States are also providing financial assistance for the PwD and elderly under various schemes. The following tables show the existing State Government disability and old-age pension schemes and financial assistance in India:
Source: Compiled by authors
In light of the Coronavirus crisis, it was announced that the Centre will provide three months of pension in advance to poor senior citizens, differently-abled and widows under its National Social Assistance Program (NSAP). Further, under the Pradhan Mantri Garib Kalyan Yojana (PMGKY), the Union Finance Minister announced an ex-gratia of Rs 1,000 over three months in two instalments for poor senior citizens, disabled communities and widows.
The National Platform for the Rights of the Disabled (NPRD) and various groups and experts has expressed dismay as the ex-gratia amount is “very meagre” and “grossly inadequate”.
The central government also issued instructions to all states and union territories to ensure that caregivers of PwD were able to reach them during the three-week lockdown (now extended). In March the Ministry of Social Justice and Empowerment issued instructions to implementing agencies for senior citizens such as Old Age Homes, Regional Resource Training Centres and Rehabilitation Centres, to provide the elderly with special medical attention and care.
The DEPwD or Divangjan has issued “Comprehensive Disability Inclusive Guidelines” The Ministry of Health and Family Welfare has also published a Health Advisory for Elderly Population of India during COVID-19.
To mitigate the effects of the lockdown, various state governments have focused on the financial assistance being given to the PwD and pensions to the poor elderly population. For instance, the Bihar state government is providing three-month advance pension through Direct Benefit Transfer to pension holders under the Divyang scheme, among others. The Delhi government has doubled the pension amount for widows, differently-abled and the elderly to Rs. 5000 per month.
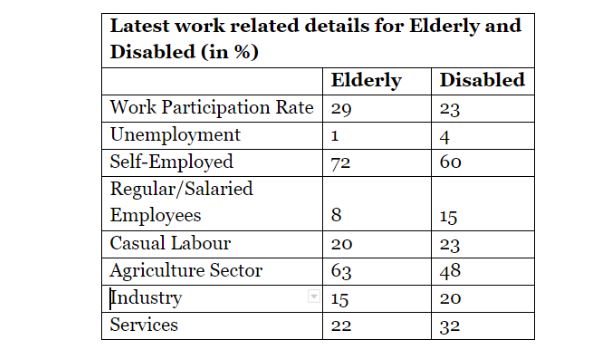
Elderly, PwD and Work Participation During COVID-19
As per the latest information available from the Periodic Labour Force Survey (PLFS) 2017-18, almost one out of three elderly people are engaged in some economic activities for their survival (29%). The work participation rate among poorest 40% households is slightly higher, indicating more vulnerability among those elderly people who belong to poor households.
Almost three-fourths of vulnerable elderly people are working in low productive and subsistance agriculture (73%) sector followed by construction (7.4%) and hotel, trade and restaurant (6.8%).
This means that almost 87% of elderly population belonging to the bottom forty percent of the households on the economic ladder are vulnerable and in the worst conditions. They need urgent assistance, particularly in the absence of any alternative livelihood opportunities.
Source: PLFS, 2017-18 and NSS, 2018; computed by Authors.
On the other hand, according the NSS Survey, 2018, only 23% of adults with disabilities are working, while just 4.2% are unemployment. This indicates that over three-fourths (77%) of people with disabilities are depends upon other family members and government welfare schemes for their livelihood and survival.
Of those employed, the majority are involved in low productive agriculture sector, low income self employment and casual work. So, one can say, that even the majority of people with disabilities who are employed are engaged in informal or low paid activities and are likely to be heavily affected by the lockdown.
The Way Forward
With mandatory distancing advised for senior citizens, they are rapidly experiencing a plethora of changes and an exacerbation of pre-existing troubles: loneliness, restricted mobility, and a lack of financial security to name a few.
The India Ageing Report – 2017 by the United Nations Population Fund (UNFPA) estimated that by 2030 around 12.5% of our population will be 60 years and older and by 2050 one-fifth of India’s population will be aged.
It further highlighted their multiple vulnerabilities and shone a light on the status of elderly women as well, who are further at risk due to a longer life expectancy and the absence of a proper social security network.
Knowing this, and witnessing the current crisis, it is only prudent to provide opportune increased support to the vulnerable elderly and disabled population.
Further, alongside, the government urgently needs to set aside a corpus of its resources for the disability sector to provide them immediate relief.
Any plan initiated should be equally inclusive for the women and transgenders with disabilities and old age.
Organisations of Persons with Disabilities (OPDs) and disability rights or advocacy groups should be involved to harness their expertise and to play important roles in raising awareness and disseminating information among the PwD in addition to advocating for disability-inclusive responses to the COVID-19 emergency.
Coordinated efforts by all stakeholders, governments, communities and civil society organisations are extremely crucial at this juncture, with active support from the citizenry.
Affirmative actions to decontaminate these disabled communities from the perils of coronavirus can have a far-reaching impact.
These suggestions have been written keeping in mind the steps to be taken immediately during the continued lockdown period.
The NSAP has a criteria of 80% and above disability for you to be eligible for the benefits under the scheme. According to the NSAP dashboard, there were 2.09 crore pensioners under IGNOAPS (the Indira Gandhi National Old Age Pension Scheme) and 17.3 lakh pensioners under the IGNDPS (Indira Gandhi National Disability Pension Scheme) in 2019-20.
During these tough times, it is advisable to relax the eligibility criteria and expand the reach, and provide more than the ‘meagre sums’ – as suggested from the measures announced under PMGKY – so individuals are, at the least, able to fulfil their monthly basic needs.
As the number of individuals in need increases due to the fallback in livelihood due to the pandemic and the lockdown, it is necessary to take these schemes further by increasing the scope of coverage and provide assistance to more number of beneficiaries.
The budget allocation for pensions to the poor elderly and disabled populations has remained static or increased only marginally during this crisis.
The 2020-21 budget for NSAP should be appropriately increased – ideally doubled – to match a corresponding increase in the targeted number of beneficiaries.
Access to welfare schemes for people with disabilities and the elderly should be streamlined to eliminate mental agony, physical struggle and delays in obtaining financial assistance.
Red-tapism and corruption should be checked.
The central government should also strengthen other financial inclusion and social transformation schemes like “JAM-Trinity” and make them more convenient so as to use technology for the convenience and not the other way around.
Cash assistance must be provided along with special provisions under the Public Distribution Scheme for the PwD and elderly on an urgent basis.
To combat the pandemic, awareness and information dissemination are of utmost importance. Users and reporting entities of print, electronic and social media should be instructed on and sensitised about the special needs of the elderly and PwD.
Video conferencing, telemedicine and telephone conversations can be adopted by doctors to contact patients with disabilities.
An online information and grievance portal should be devised, inclusive of all types of disabilities, and the challenges specific to old-age and related ailments, with special psychological counselling services. It should be centred on accessibility and ease of use, with simple input requirements.
This is imperative to minimise the need for human intervention and dependence, and to promote self-reliance.
Information can and should be disseminated with disability- and elderly-inclusive practices of publicity (using sign language, voice assistance, minimalistic interface and others).
Information should be made accessible also in the regional languages and the information should be disseminated through the coordinated efforts of the government, NGOs and civil societies even after the lockdown is lifted.
Governments should ensure accessible study materials and lesson plans for disabled students who do not have access to the internet. Without government support, parents or caregivers may struggle to provide the full range of services their children may receive in schools.
Access to aids, devices and necessary mobility and communication equipment to the PwD and elderly during the lockdown should also be ensured.
The bureaucracy in charge of the welfare of the PwD must be sensitised and streamlined. Those states still without a state commissioner for PwD, or the chief commissioner for PwD as per DEPwD guidelines, must be instated urgently. In fact their appointment must precede with a background check on their understanding of the sensitivity, support, knowledge, training and motivation of the challenges and needs of the PwDs. The appointment of specialists/ experts possessing these traits can also be explored for this position.
The caregivers of these vulnerable sections must be sensitised and trained and it must be ensured that they do not face any troubles in reaching out to their dependents. For this purpose, passes should be arranged; provisioning of e-pass for this purpose should be incorporated be one of the options.
Precautionary measures and increased financial assistance should be provided to caregivers. Residents’ Welfare Associations can volunteer to carry out tasks such as wellness checks on the elderly and people with disabilities if there is a need for the same.
Communities need to come together and extend their support in combating loneliness in isolation and assist in a linkage to information and communications technology, with assistance and teaching.
To conclude, in the prevailing health exigency, the elderly and people with disabilities face compounded challenges. It is the responsibility of governments at all levels to work in tandem with each other and with civil society organisations to provide increased, emergency funding for programs that allow seniors and PwDs to remain healthy, anxiety-free and safe at home.
We believe that through concerted action, India could set an example before the world and successfully contain this humanitarian crisis.


Dr. Arjun Kumar, Prof. Manish Priyadarshi, Dr. Simi Mehta, Prof. Balwant Singh Mehta, Prof. I C Awasthi, Prof. Soumyadip Chattopadhyay, Prof. Shipra Maitra, Dr. Indu Prakash Singh, Raj Kumar, Ritika Gupta, Anshula Mehta, Dr. Kahkashan Kamaal, Baikunth Roy, Dr. Dolly Pal, Pooja Kumari and the Impact and Policy Research Institute (IMPRI) Team


{kind=link}